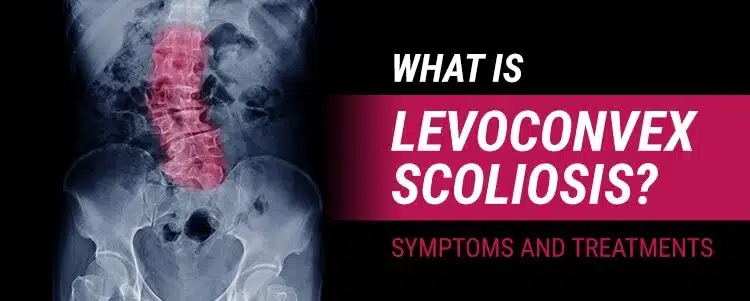
The term ‘levoconvex scoliosis’ is something you might see written in a radiography report. Put simply, it’s a medical term that classifies the condition by explaining in which direction the scoliosis curve bends. Levoconvex scoliosis is a form of the condition where the patient’s spinal curvature is located in the thoracic spine (middle back) and bends to the left. Curvatures that bend towards the left side of the body, where the heart is, are considered atypical.
The spine plays a huge role in regulating the body and facilitating its movements. It works in tandem with the brain to make up the body’s central nervous system. When a condition develops that impacts the spine, its effects can be felt throughout the body. Before we get into the details of scoliosis development along different sections of the spine, let’s first explore some basic spinal anatomy.
Basic Spinal Anatomy
The spine is made up of three main sections: cervical (upper back and neck), thoracic (middle back), and the lumbar spine (lower back). Below the lumbar spine is the sacrum: a bone that’s part of the pelvis.
The individual bones that make up the spine are called vertebrae. In a healthy spine, these are stacked on top of one another like bricks. If one is misshapen, this throws off the alignment of the entire spine.
The cervical spine consists of 7 vertebrae; the thoracic spine has 12, and the lumbar spine has 5. The thoracic spine is the most common site for scoliosis to develop, and given that it is the largest spinal segment consisting of the most vertebrae, this makes sense. The spine is made up of 33 vertebrae in total.
A normal spine has three healthy curves, and these curves are there for a reason.
The Spine’s Healthy Curves
Have you ever stopped to wonder why the spine is curved in the first place? The spine is curved because it’s stronger that way. It’s better able to absorb force and distribute its impact evenly along the spine. It also helps facilitate mobility and flexible movement.
When you look at a spine from the side, you can see it has gentle curves that make a soft ‘S’ shape. These natural curves work together almost as a type of coiled spring: capable of compressing to absorb shock and impact while still facilitating a wide range of motion throughout the spine.
Healthy backs have three natural curves:
- An inward (concave) curve of the cervical spine at the neck
- An outward (convex) curve at the thoracic spine (middle back)
- An inward curve at the lumbar spine (lower back just above the sacrum)
As important as these healthy curves are, there are a number of different unhealthy curves that can develop and throw off the biomechanics of the spine.
When a Spine Loses its Healthy Curves

When a person develops scoliosis, this means there is a loss of the spine’s healthy curves. As the spine loses its healthy curves, they are replaced by bad curves, and as scoliosis is a progressive condition, the abnormal sideways curvature becomes structural and is virtually guaranteed to worsen over time.
When scoliosis is first diagnosed, it’s classified based on a number of patient characteristics and the results of their scoliosis X-ray: age of patient, type of curvature, location of the curvature, and in which direction the curve bends.
Just as there are different sections of the spine with different healthy curves, there are a number of unhealthy curves that can also develop.
Dextroscoliosis
In typical scoliosis cases, the spine’s abnormal sideways curvature will bend to the right, away from the heart; this is referred to as a dextrocurvature.
Dextroscoliosis is one of the most common types of scoliosis curvatures and depending on how severe it is can give the spine a pronounced ‘S’ or ‘C’ shape, rather than the soft ‘S’ of a healthy spine.
Dextroscoliosis mainly affects the thoracic spine and is commonly diagnosed in adolescents between the ages of 10 and 18: adolescent idiopathic scoliosis. Its onset is often triggered by the first big growth spurt of puberty.
Common symptoms of Dextroscoliosis to look for include postural changes that can range from subtle to overt, depending on condition severity: uneven shoulder height, rib arch, uneven hips and waistline, and changes to gait.
The more severe a condition is, the more noticeable these symptoms can be and the more asymmetric the body can appear. Often, there aren’t many functional deficits or noticeable symptoms in milder conditions, especially when it first develops, and this is why early detection can be a challenge.
It’s when the condition is left untreated and progresses unimpeded that it can start to produce the type of symptoms that would be noticed by an average person, not a scoliosis specialist who knows what to look for.
Dextroconvex Scoliosis
Also known as ‘lumbar dextroscoliosis’, dextroconvex scoliosis commonly causes an ‘S’ curvature to form in the lumbar region.
Scoliosis curvatures have a huge range in severity and can be measured at anywhere from 10 to 150 degrees. The measurement, in degrees, of how much an abnormally-curved spine deviates from a straight alignment is known as the Cobb angle. The higher the Cobb angle, the more severe the condition is, and the more likely it is to produce noticeable symptoms like changes to posture, gait, and cause discomfort or mobility issues.
Mild dextroscoliosis would be considered a curvature that measures around 10 or 20 degrees, and the higher up the Cobb angle gets, the more severe the condition is classified.
Similar reading: S-Shaped Scoliosis: What Is It?
Thoracic Dextroscoliosis
Thoracic dextroscoliosis refers to an abnormal spinal curvature that develops in the thoracic spine and curves to the right.
Mild forms of the condition typically refer to Cobb angle measurements of 10 to 20 degrees. The thoracic spine is the most common site for scoliosis to develop and this location is commonly associated with a rib arch characteristic of the condition.

Levoscoliosis
Levoscoliosis is the opposite form of dextroscoliosis and is considered atypical because the sideways spinal curvature bends to the left, instead of the right: referred to as a levocurvature.
This type of scoliosis most commonly affects the lumbar and thoracic spine. Just as all forms of scoliosis, levoscoliosis can range from mild to moderate and severe. The most severe cases have the potential to cause related organ and lung-impairment issues.
When I see a curvature that bends to the left, this is a red flag. When I see this, I have to rule out any underlying pathology before moving forward with treatment. When I see an atypical scoliosis, it is most often a secondary complication of another medical issue or disease. Possible causes could be congenital (a hemivertebra present at birth), a neuromuscular disorder such as muscular dystrophy or cerebral palsy, trauma-induced, or the presence of tumors.
Also known as ‘thoracic levoscoliosis’, levoconvex scoliosis affects the thoracic section of the spine but can also develop along the lumbar spine.
Levoconvex scoliosis is simply a further specification of levoscoliosis as it specifies that it’s the curve’s outer edge (convex side) that curves to the left. The term ‘concave’ refers to the inner edge of the curve.
Lumbar Levoscoliosis
If a person is diagnosed with lumbar levoscoliosis, this means they have developed a curvature in the spine’s lumbar region that will likely take on a hard ‘C’ shape. The lower spine’s vertebrae are affected, and the curve bends to the left.
Atypical Scoliosis
As you can see, scoliosis is a complex condition that can take many forms. From mild to severe, it can develop at any age and at any location along the spine. While some forms are more common and simpler to treat, all forms need active treatment to manage the condition’s progression.
When it comes to atypical forms of the condition such as levoconvex scoliosis, where the curvature bends to the left, as I said earlier, this is a red flag.
Most scoliosis curvatures bend to the right, away from the heart, so if an X-ray image shows a curvature bending to the left, I know there is likely another issue causing the scoliosis, and that underlying issue has to be addressed first.
Congenital Scoliosis
In congenital scoliosis, this means there is a malformed vertebra (hemivertebra) that was present at birth. If you think of the individual vertebra of the spine as rectangular building blocks that sit on top of one another, a malformed vertebra can be triangular in shape and cause the spine to slip out of alignment.
Neuromuscular Scoliosis
Neuromuscular scoliosis develops as a secondary complication of disorders of the nerve and muscular systems such as cerebral palsy and muscular dystrophy. These conditions impair the ability to control the muscles that stabilize and support the spine.
Trauma-Induced Scoliosis and Tumors

An especially common cause of adult scoliosis, extreme trauma experienced by the spine can cause injury that results in an abnormal curvature developing.
Tumors can also develop along the spine and apply pressure that pushes the spine out of alignment. In these kinds of cases, patients are referred to specialists experienced with tumor removal and would likely undergo treatment to try and first shrink the tumors, or undergo surgery to have them removed.
In the above scenarios that are considered atypical forms of scoliosis, the scoliosis has developed as a secondary complication of a larger medical issue. In these cases, I would assess their scoliosis and likely refer them to someone who specializes in the underlying cause of the condition, prior to addressing the structural component of the scoliosis itself.
Scoliosis Classification
When we classify a patient’s condition, we are finding the condition’s most important characteristics and their condition name reflects these variables.
Age of Patient
Age of patient tells us their likely level of health and fitness, in addition to the condition’s most likely rate of progression.
While there is no easy formula that can be applied to determine a patient’s rate of progression, we know that age plays a big factor.
As growth is the number-one trigger for progression, we know that the more growth a person has yet to go through, the higher their risk of progression is going to be. This is why the most common age of diagnosis is between 10 and 18: when adolescents are entering into the stage of puberty marked by rapid and unpredictable growth spurts.
Once a patient reaches skeletal maturity, that trigger for progression has been removed, so likely rates of progression will slow.
Age also tells us whether pain is likely to be a notable part of the patient’s experience with the condition. In adolescence, the spine is constantly lengthening because of growth; this makes it impervious to the compressive effects of the curvature.
When a person reaches skeletal maturity, that lengthening motion stops, and now, the spine becomes vulnerable to the compression caused by the abnormally-curved spine. It’s most often pain that brings adults in to see me, and commonly, adults with scoliosis had it in adolescence too but were unaware of it. It’s not until they stop growing that their condition starts to show noticeable symptoms leading them, finally, to a scoliosis diagnosis.
Type of Curvature
Type of curvature is another big classification point. ‘Type’ mainly refers to the condition’s cause, if known. In the vast majority of cases, they are classed as ‘idiopathic’, meaning no known single cause.
In the above mentioned atypical forms of scoliosis, these known causes classify the condition and indicate the type of treatment approach that will be needed.
Location of Curvature and Direction of the Bend
The location of the curvature is important because it tells us where along the spine our treatment efforts need to be focused. A cervical designation tells us the upper back is the location of the curvature. Thoracic scoliosis tells us it occupies the middle back, and lumbar scoliosis tells us the lower back is the site of the curvature.
The direction in which the curvature bends is also an important designation because it tells us if we are dealing with a typical or atypical case. As is the case with many medical terms, ‘levo’ and ‘dextro’ are prefixes from Latin words.
‘Levo’ means ‘left’ and ‘dextro’ means ‘right’. Therefore, if a person is diagnosed with levoscoliosis, this means their scoliosis is atypical and curves to the left; if a person is diagnosed with dextroscoliosis, this means their curvature is typical and bends to the right, away from the heart.
Severity of the Curvature
Perhaps the most important classification point, severity of the curvature tells us how extreme the abnormally-curved spine is. This is very important because, as we’ve discussed, scoliosis develops across a wide severity spectrum ranging from mild and moderate to severe.
Where a patient’s condition falls on this scale tells us how hard we need to work to restore as many of the spine’s healthy curves as possible. It also indicates what symptoms they are likely to experience and what the condition’s likely rate of progression will be.
Curvature severity is determined by the patient’s Cobb angle: a measurement obtained via X-ray taken at the apex of the curve from the most-tilted vertebrae. This measurement tells us how far from a normal alignment the scoliosis spine deviates.
- Mild scoliosis: Cobb angle measurement of 25 degrees or less
- Moderate scoliosis: Cobb angle measurement between 25 and 40 degrees
- Severe scoliosis: Cobb angle measurement of 40+ degrees
I’ve treated patients with 100+ degree curvatures, so you can see how significant this range can be and how important it would be in classifying a patient’s condition.

Conclusion
There are a lot of confusing medical terms thrown around when diagnosing and assessing medical conditions and diseases. When a person is hearing their diagnosis for the first time, this can be very overwhelming. It’s hard to take in and process everything you or a loved one are being told, especially when there are complex medical terms to contend with.
Understanding some of the basic medical terms that classify scoliosis can be very helpful in processing the condition’s various characteristics.
If you hear a designation of levoconvex scoliosis, you know this refers to atypical cases where the scoliosis curvature bends to the left. Typical scoliosis curves bend to the right, away from the heart, so a curve that bends to the left suggests another pathology at play.
Here at the Scoliosis Reduction Center®, we’ve treated all forms and types of scoliosis. In atypical cases, once the underlying cause of the condition has been addressed, we can start working towards achieving a curvature reduction on a structural level and restoring the spine’s healthy curves.



